
Creating a new smile with your own hands: direct resin veneers
By Dr. Eloy Burga Noriega, DDS
I. Introduction
People´s awareness of esthetic dentistry is no more under discussion; it´s a fact. Ordinary men and women, not only media stars, want radiant smiles. Esthetic enhancement of dentition can be done through a great array of procedures and different degrees of invasiveness.
Which is the best procedure? The expert practitioner is able to determine which is the best solution through an accurate diagnosis. Generally speaking, patients prefer the less invasive treatments although some of them imply that the work will need to be redone some time in the future.
«We all know that everything we do in dentistry has a lifespan and at some point most, if not all, of the restorations we place will need to be replaced.» (1)
Direct bonding of composite resin can provide excellent and extremely conservative esthetic results. For decades, direct resin veneers have been an important part of the services provided by cosmetic dentists, but the results are now better because of the improvements in many areas. For example, the incorporation of a variety of new shades makes it possible to create virtually life-like restorations. To be able to simulate the teeth structure in all their characteristics, of course, does not depend only upon the quality of the material or the equipment. The dentist´s hands and his of her artistic sensibility and skills play an irreplaceable role.
Although we now have the tools to create beautiful restorations with our own hands, some practitioners hesitate to recommend direct composite veneers because they don´t feel sure about their artistic eye, have not developed the skills needed to perform such an artistic work or have acquired a dependence on laboratories that they find difficult to brake. This must not prevent them to inform the patient about all the alternatives. Of course, directly bonded composite veneers are not a magical solution for every case. In fact, «too many dentists are utilizing veneers instead of orthodontics»(2).
The main advantages of directly bonded composite veneers are, little or no tooth preparations, easy to repair intraorally should it chip or fracture, and reversibility. Another advantage is that «Composite resin will not cause iatrogenic wear of opposing structures». (3) The disadvantage is that they may not prove to be as durable as some indirect alternatives.
Direct resins have been called «the flagship of cosmetic dentistry» (4). To enhance or rehabilitate a smile using directly sculpted and polished composite resins is one of the most challenging treatments. It requires an exceptionally high level of skill, a great deal of concentration, and full control over the results.
For these and many other reasons I believe composite resin should be included in the menu of services provided by a cosmetic dentist who strives to conquer excellence in this field.
| 1 | Spoor, Rhys. «A Conservative Approach to Changing the Smile with the Maxillary Incisors». Odontología Estética. Mayo-Julio 2006. p. 13. | |
| 2 | Christensen, Gordon. «Esthetic Dentistry: State of the art». General Dentistry. Nov. 2007. Vol Nº 55. Nº7. p. 611 | |
| 3 | Nash, Ross W. «Finding Closure». Dental Products Report. August, 2006. p. 82. | |
| 4 | Hastings, James. «Case Selection: Case Type V, Sir or More Direct Resin Veneers». The Journal of Cosmetic Dentistry. Volume 21. Nº 3. Fall, 2005. p. 102. |
II: History

(Figure 1) Pre-operative view of patient´s smile. 1:2
The patient was a healthy 14 year-old girl with no medical contraindications for treatment. Due to her congenitally missing laterals, she had received orthodontic treatment since she was 11 years old to move her canines into lateral positions with subsequent movement of all other teeth forward.
The orthodontic treatment was successful, but when the braces were taken off it was obvious that something must be done to correct the shape and improve the look.
The girl and her parents have two chief complaints; the canines do not look natural in that position and there was a rotation of the two central incisors which also showed diastemata. There were asymmetrical spacing in certain areas.
When her family dentist presented the patient with the option of an orthodontic consult, she refused to consider again the use of braces. Her parents supported her position and stated that they were looking for an alternative treatment.

(Figure 2) Pre-Operative view patient 1:2
III. Treatment plan
The treatment plan included a comprehensive examination. Records were taken to help develop the treatment plan, including a full-mouth series of radiographs and a set of 35 mm preoperative photographs showing all necessary views.
Clinical data study models and a bite registration were performed. Preparations were performed on the model and a wax-up was completed.
After a lengthy discussion of treatment modalities, with the goal of creating the illusion that the canines were actually laterals, the patient and their parents chose the most conservative one, which required minimal preparation of teeth 6,8,9, and 11 and application of direct veneers in the form of composite resin.
IV. Procedure
Preparation
Teeth 6, 8, 9, and 11 were prepared across the facial and proximal surfaces with minimal tooth enamel removal. No anesthesia was needed.
 Figure 3
Figure 3

Figure 5
 Figure 4
Figure 4

Figure 6
Bonding
Composite shade AO2 was applied to the proximal areas. An additional increment of a BW, A1, B1, WT, CVT, and NT shade was delivered to the tooth, sculpted using a thin metal-blanded instrument and then contoured. I used a sixth-generation bonding agent with a self-etching primer. See figures 7 and 8.

Figure 7

Figure 8
This case required multiple stages of composite applications. The incisal edge was left inrregular trying to create a natural translucency due to light transmission.
A sable brush with a slight film of resin was used to smooth the facial surface of the composite veneer.
 Figure 9
Figure 9
A yellow tint was applied vertically on the tooth to add a tridimensional effect to the restoration. After a series of layers, two layers of shade WT were applied onto the entire facial surface of the restoration.

Figure 10
Contouring and polishing
The lingual contouring was initiated with a pear-shaped carbide bur and the primary anatomy facial contouring with Dura green stones (CN1). See figures 11 and 12.
.
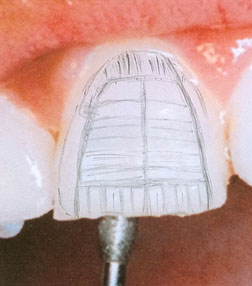
Figure 11

Figure 12
A metal diamond-coated strip was eased into proximal areas to remove the slight excess of composite. See figure 13

Figure 13
Then the facial surface was sculpted by using finishing burs (Composite and Polishing Kit – Brasseler)

Figure 14
When all teeth were completed in general shape, they were cut back to create developmental grooves. A shaped diamond was used to create internal mamelons. In this way a reflective and deflective surface was developed, creating shadowing and light reflecting for a natural-looking restoration.
The gingival margin was thinned with an eight fluted Brasseler carbide bur. The lingual surfaces were contoured with football shaped burs.
The proximal, facial, and incisal angles were finished using the Super-Snap Rainbow Kit Polishing System. The disks were used sequentially according to grit, ranging from coarse to extra fine. See figure 15.

Figure 15

Figure 16
After taking a series of photographs we made another appointment to refine and complete the case.
In order to achieve a beautiful esthetic result, some minor changes in contour were made. The restorations were polished using finishing and polishing strips. Neither subsurface bubbles nor debris were observed.

Figure 17 : Micro and Macro textures
The interproximal areas were polished using aluminium oxide polishing strips. See figure 18.

Figure 18 – 1:1

Figure 19 – 1:1
The surface texture after treatment has a smooth and shiny luster, achieved using flexicup system. The final gloss was achieved with a polishing brush and a polishing paste.
Notice the natural-looking restorations with surface morphologic characterizations. The micro and macro textures give the restorations extremely good light transmission properties. The tiny grooves and the lobes simultaneously present optimize reflection and refraction.

Figure 20 : Note the natural enamel-like
shine achieved – 1:1

Figure 21 : Pre-Operative view of patient´s smile. 1:2

Figure 22 : Post operative view of patient´s smile. 1:2

Figure 23 :Before; right lateral view.

Figure 24: After; right lateral view.

Figure 25: Before ; left lateral view.

Figure 26: After; left lateral view.

Figure 27: Pre-treatment view shows a strained facial expression.

Figure 28: The smile says it all..
V. Conclusion
It is not easy to perform direct composite veneers in a way that truly mimics nature. It is in fact difficult to achieve a natural-looking smile, unless the dentist is an expert with a highly developed artistic eye.
In fact, many dentists do not have another alternative than to place all-ceramic restorations, depriving some patients of a more conservative treatment that would be the treatment of choice.
Of course, in some circumstances a non-ceramic approach is not possible, but in this case due to the patient´s age and her strong willing for a conservative treatment, direct composite veneers were a must.
-
- Christensen, Gordon J. Esthetic dentistry: state of the art. Journal of the Academy of General Dentistry . 2007
- Dietschi, D. Free hand bonding in the esthetic treatment of anterior teeth: Creating The illusion. 1997
- Fahl, Newton. Direct Indirect composite veneer: A case report. 1996
- Hatai y. Reproducing nature: smile design. LVI Visions 2008 .
- Mopper kw. Renamel restorative system Clinical brochure. Chicago, IL; Cosmedent.
- Mopper KW. The art and science of free hand Bonding. Cosmedent: 2003
- Morley J, Eubanc J. Microesthetic elements of smile design : 2003
- Morley J. Elements for the preparations and finishing of direct and indirect anterior restorations. Contemp Esthet dent.
- Okuda WH . Achieving optimal aesthetics for direct and indirect restorations with Microhybrid composite resin. 2005.
- Peyton JH. Finishing and polishing techniques: Direct composite restorations. 2004
- Spear FM. Kokich VG. A multidiciplinary approach to esthetic dentistry. 2007
- Spoor, Rhys. The use of direct composites in the conservative esthetic correction of the anterior dentition. Journal of Cosmetic Dentistry. American Aademy of Cosmetic Dentistry.
- Terry D. Creating form and color: Creative with Direct Composite Resin ; 2002
Este artículo es propiedad intelectual del Dr. Eloy Burga Noriega y menciona procedimientos que se realizaron en Cosmética Dental Burga.
Se autoriza su reproducción total o parcial, con la debida mención de su fuente.
